This week’s post is from Dr. Michael Bertaume, an “anthroengineer”– combining studies of anthropology and mechanical engineering perspectives. This post is about his team’s scientific paper just published here. If you would like to write for Anatomy to You, get in touch via Facebook or Twitter.
The foot bone’s connected to the ankle bone,
The ankle bone’s connected to the leg bone,
The leg bone’s connected to the knee bone…
We are taught anatomy early in life, and told that the human skeleton has 206 bones. When asked what bones make up the “knee bone,” most people say the femur, patella, and tibia. But some people have more bones in their knee: sesamoid bones. And few people know that the average number of bones in human skeletons… is changing…
The fabella is a sesamoid bone located in the lateral head of the gastrocnemius muscle, behind the lateral femoral condyle (Figure 1). It is common in non-human mammals, but human prevalence varies from 3-87% [1,2], making it a normal anatomical variant. In 1918, an average of 11.22% of human knees, worldwide, had fabellae, with bilateral cases (one/knee) being more common than unilateral ones (one/person). But today, the average prevalence is 39.08%. Why the increase? And why is the fabella more common, when other sesamoid bones in the hands and feet are not [3]? The clinical and evolutionarily importance of the fabella makes this an important question to answer.
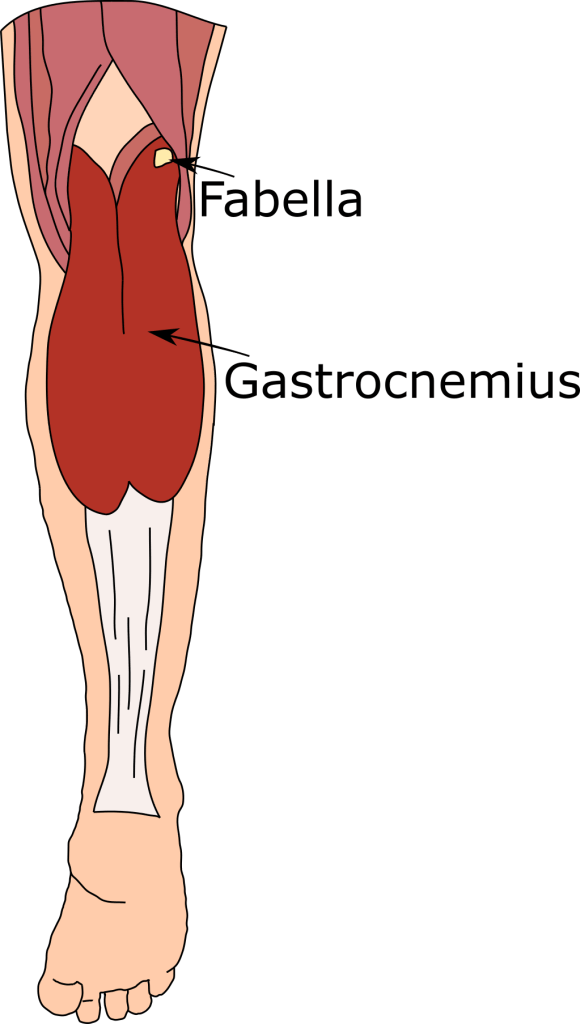
Figure 1: Fabella, in the lateral head of the gastrocnemius. Lower leg shown in posterior (rear) view.
Clinically, the fabella is associated with knee diseases (e.g., osteoarthritis, nerve palsy, popliteal artery entrapment syndrome), can cause pain on its own (dislocation, fracture), and can cause generalized discomfort (fabella syndrome). It can also be problematic during total knee replacements, as replacement knees lack the fossa (depression) sometimes found on the posterior side of the lateral femoral condyle which stabilizes the fabella [4,5]. While problems can be managed conservatively, fabellectomies are common, and appear to have no long term adverse effects (although no studies have quantified the effects of fabella removal on the knee).
Fabellar function, in humans, is largely unknown. In quadrupedal mammals, like monkeys, it appears to function like the patella, increasing muscle mechanical advantage. In human, straight-legged, bipedal gait, this may not happen, as the fabella may stop articulating with the femoral condyle as the knee bends. The presence of the fabella in humans is interesting, as it is rare in great apes compared to other primates (Figure 2) – updated studies with larger primate samples are sorely needed to understand the evolution of the fabella in hominoids (apes & kin).
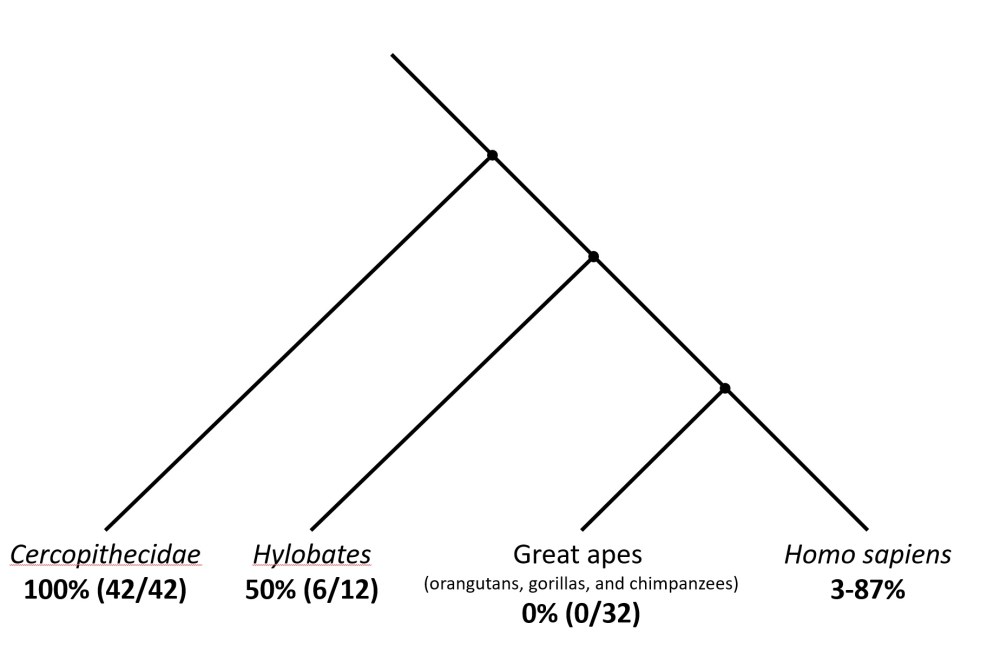
Figure 2: Prevalence rates of fabellae in primates, mapped onto a phylogeny (family tree). Over 60 studies have reported on fabella prevalence rates in Homo sapiens, totalling over 20,000 knees. Figure modified from [6].
Changes in phenotype, like fabella presence, can have genetic and/or environmental causes. Genetics are likely not responsible for the increase in fabella prevalence, as increases are happening both within and across genetically distinct populations (Figure 3). If not genetic, environmental?
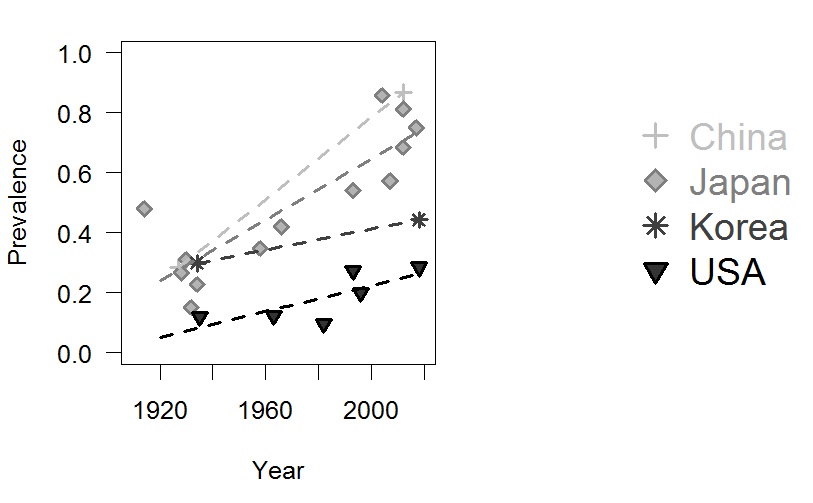
Figure 3: Prevalence rates (1.0 = 100%) for countries with prevalence rate studies before and after 1960. Dotted lines connect the two studies for China and Korea, and are Pearson’s linear regressions for Japan and the USA. Figure from [3].
Few environmental factors have affected all human populations over the last 100 years, but one that has is nutrition. The average human, today, is better nourished, meaning people today are taller and heavier. This likely increased: a) tibial length, creating a larger moment (torque or rotational force) about the knee, and b) gastrocnemius size, increasing muscle force. Together, these factors may be producing higher mechanical stimuli in the tendon of the lateral head of the gastrocnemius. As sesamoid bones tend to form in response to mechanical stimuli, this increased stimuli may be signalling fabella ossification.
Not all people have fabellae, however, as there is likely a genetic component controlling the ability to form a fabella: the strongest evidence for this is populational differences in fabella prevalence rates [3]. But for those that can form a fabella, this increased mechanical signal may be causing them to ossify [3].
References:
- Zeng S-X, Dong X-L, Dang R-S, Wu G-S, Wang J-F, Wang D, et al. Anatomic study of fabella and its surrounding structures in a Chinese population. Surg Radiol Anat. Springer-Verlag; 2012;34: 65–71. doi:10.1007/s00276-011-0828-4
- Silva JG, Chagas CAA, Torres DFM, Servidio L, Vilela AC, Chagas WA. Morphological analyisis of the fabella in Brazilians. Int J Morphol Int J Morphol. 2010;28: 105–10. Available: https://pdfs.semanticscholar.org/8b17/9afe8e34f151f963d1fc43b9889798e71874.pdf
- Berthaume MA, Di Federico E, Bull AMJ. Fabella prevalence rate increases over 150 years, rates of other sesamoid bones remain constant: a systematic review. J Anat.
- Larson JE, Becker DA. Fabellar impingement in total knee arthroplasty. A case report. J Arthroplasty. Elsevier; 1993;8: 95–7. doi:10.1016/S0883-5403(06)80114-2
- Hou W. Should we remove the fabella in total knee arthroplasy of osteoarthritis. 5th International Conference of Orthopedic Surgeons and Rheumatology. 2016. p. 74.
- Sarin VK, Erickson GM, Giori NJ, Bergman AG, Carter DR. Coincident development of sesamoid bones and clues to their evolution. Anatomical Record, 1999; 257: 174-180.
